Blog
19 Jul 2021
Plantar Fasciitis – Which is the Best Option for Treatment?
By Margaret Kraeling, DPT, CCRT
There are many different sources of pain in the plantar heel besides the plantar fascia and therefore the term "Plantar Heel Pain" is perhaps a better terminology to describe this condition.
This is often an overuse injury that is primarily due to a repetitive strain causing micro-tears of the plantar fascia but can also occur as a result of trauma.
Although the term plantar fasciitis has the ending “itis” there is a notable absence of inflammatory cells.
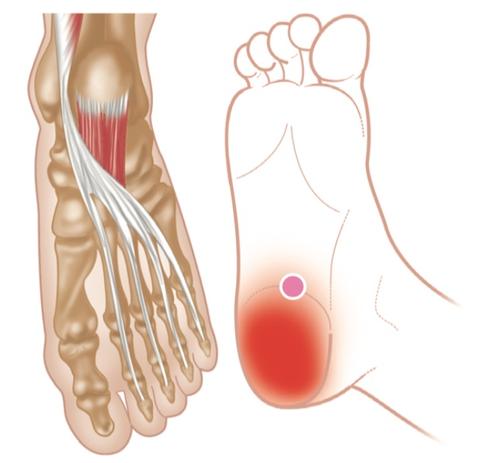
The condition is characterised by degeneration of the plantar fascia at the origin on the calcaneal tuberosity of the heel bone.
The plantar fascia is important in the biomechanics of the foot in motion, supporting the arch of the foot and providing shock absorption.
This condition is reported to account for 10 – 22% of runner – related injuries and is also seen to occur in 10% of the general population, 85% of these working adults between 25 – 65 years of age. Running has become a very popular form of exercise due to the relatively low cost of equipment and easy accessibility of free venues.

The average episode lasts more than 6 months. Most respond to conservative treatment. It is the most common foot condition treated in physical therapy clinics and in the US, it accounts for up to 40% of all patients.
There are many suggested causes and treatment for plantar heel pain. Let’s look at a few common ideas.
It is often thought that plantar heel pain is accompanied by heel spurs. Although this can be a common association it should also be noted that 32% of the people with no heel pain have a heel spur visible on x-ray.
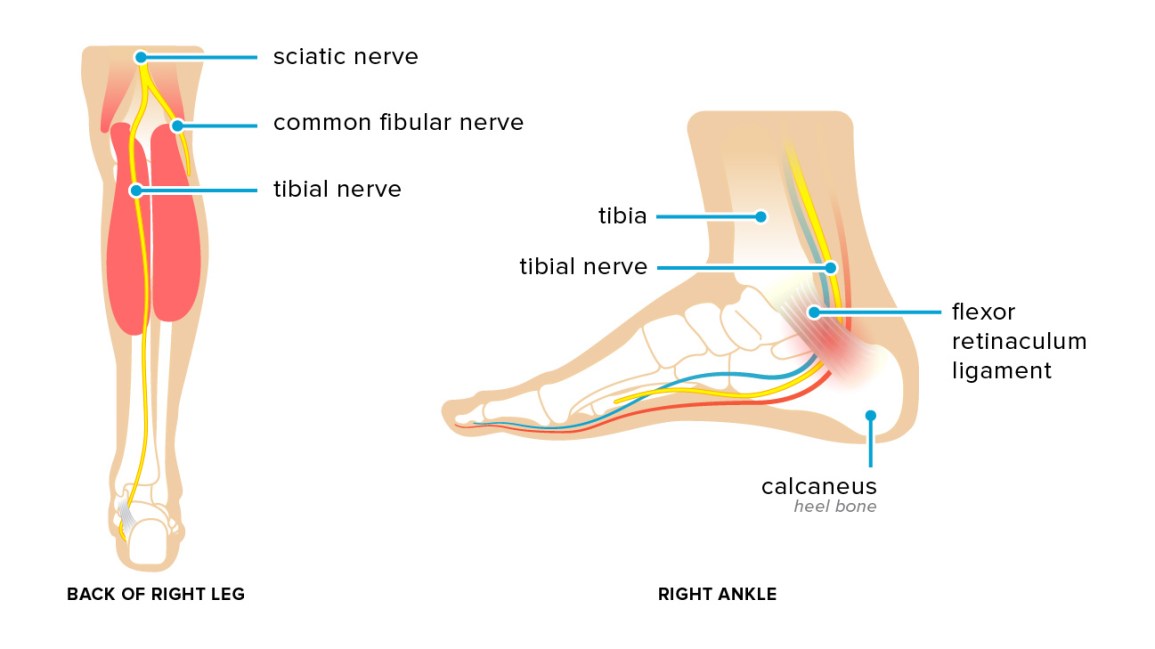
It is commonly accepted that limited mobility in the joints of the foot and ankle can contribute to this condition however studies show that muscle imbalances and tight connective tissue especially in the calf have more impact on this condition. Sometimes when limited results are being obtained with treatment, we need to also assess the tibial nerve to see if that is the cause of the heel pain.
We can often see cases where new shoes, heel cushions or orthotics fail to provide a suitable resolution. This is where we need to do a complete evaluation of these other factors that can be contributing to the patients heel pain.
After many years of treating cases of plantar heel pain (and seeing a variety of treatment approaches come and go) I have developed an approach that I find I am comfortable with. Since I am basically very biomechanically based, I always start with a structural assessment including overall posture and joint mobility. I then test for muscle imbalances in the lower extremities and connective tissue tightness.
From here I will develop and approach to address all of these with specific manual therapy techniques, exercises and connective tissue / myofascial release techniques or neural tissue techniques. My favourites as far as modalities go are shock wave and laser locally on the foot and often on tight areas in the calf muscles. I also utilize cupping or tissue distraction techniques with good benefit (although I always warn my patients that this can be uncomfortable on a tight calf muscle!).

This approach along with correctly fitting shoes will, in most cases, allow the patient to continue with their favourite activities.